Apligraf® real-world evidence.
Observational comparative effectiveness studies proved that Apligraf closes more VLUs and DFUs faster.1-3
- 50% of VLU wounds closed by week 24 for Apligraf vs 41% for Oasis (P=0.01)1
- Median time to wound closure was 24 weeks for Apligraf vs 43 weeks for Oasis (P=0.01)1
- Apligraf closed VLUs 44% faster1
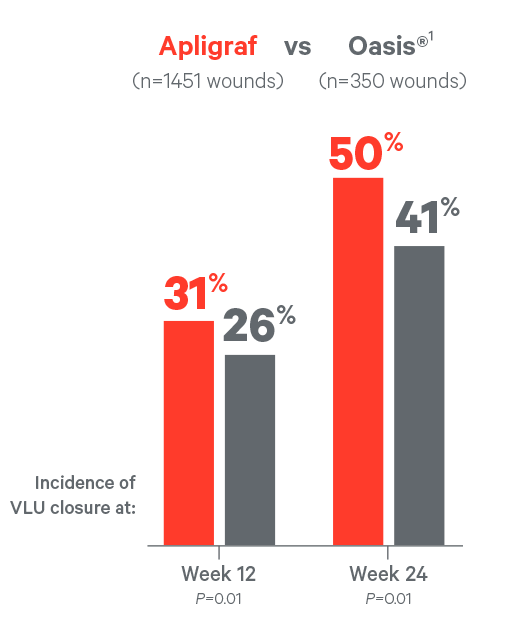
For the Apligraf vs Oasis analyses, incidence of and median time to wound closure were determined by Kaplan-Meier analysis with two-tailed log-rank test. The hazard ratio along with its 95% confidence interval (CI) and P value is based on a Cox proportional hazards regression model with one term for treatment group. Wound closure defined as an ulcer achieving an area between 0 and 0.25 cm2.
- 65% of VLU wounds closed by week 24 for Apligraf vs 41% for TheraSkin (P=0.0002)2
- Median time to wound closure was 15 weeks for Apligraf vs 31 weeks for TheraSkin (P=0.0002)2
- Apligraf closed VLUs 52% faster2
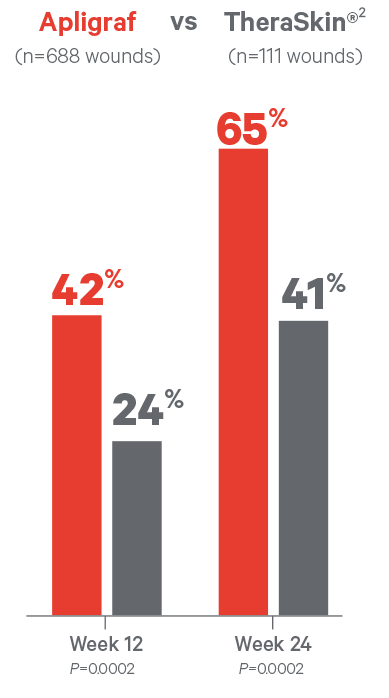
For the Apligraf vs TheraSkin analyses, the estimated incidence of wound closure and the estimated median time to wound closure are from a Cox regression model with terms for treatment, baseline wound area, baseline wound duration, baseline wound depth, and patient age at first visit. Wound closure defined as an ulcer achieving an area between 0 and 0.25 cm2.
- 55% of VLU wounds closed by week 24 for Apligraf vs 43% for PriMatrix (P=0.01)3
- Median time to wound closure was 19 weeks for Apligraf vs 30 weeks for PriMatrix (P=0.01)3
- Apligraf closed VLUs 37% faster3
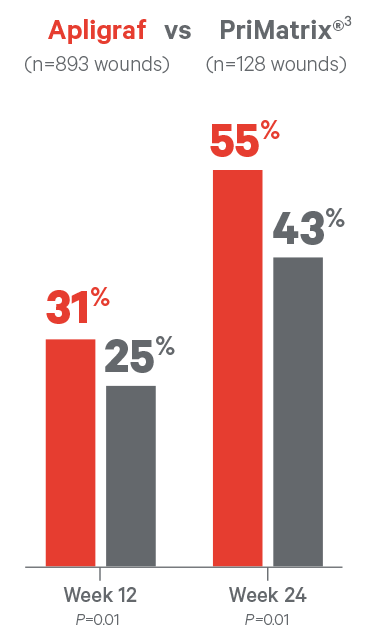
For the Apligraf vs PriMatrix analyses, the estimated incidence of wound closure and estimated median time to wound closure are from a Cox regression model with terms for treatment, baseline wound area, baseline wound duration, baseline wound depth, patient age at first treatment, sex, and body mass index. Wound closure defined as an ulcer achieving an area between 0 and 0.25 cm2.
- Incidence of DFU closure at week 12 was 48% vs 28% for EpiFix (P=0.01)4
- Median time to wound closure was 13 weeks for Apligraf vs 26 weeks for EpiFix (P=0.01)4
- Apligraf closed DFUs 49% faster4
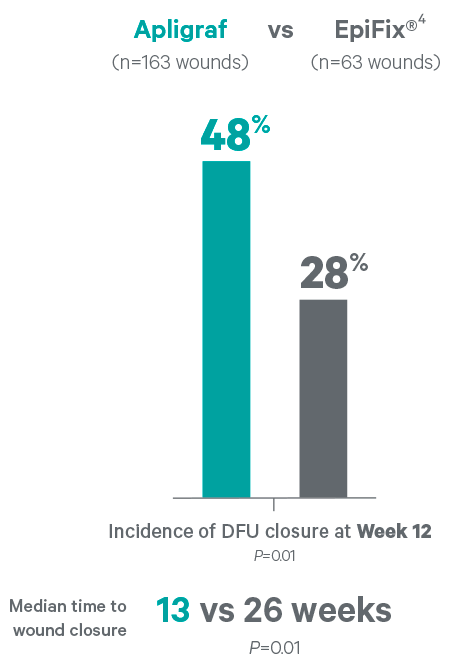
Estimated incidence of and median time to wound closure and P value are from a Cox regression model with terms for treatment, baseline wound area, duration, depth, and location. P=0.01. Wound closure defined as an ulcer achieving an area between 0 and 0.25 cm2. Although more patients received Apligraf treatment vs EpiFix in the database, there were no preferential exclusion/inclusion criteria applied. Additionally, the statistical methods employed ensure no bias for number of patients in either treatment group. The primary analyses were frequency of wound closure by week 12 and week 24, and median time to wound closure. As patients with healed wounds do not always follow up, wound closure was defined as an ulcer achieving area ≤0.25 cm2.
*Effectiveness is the extent to which an intervention produces an overall health benefit in routine clinical practice (real-world situations). Effectiveness studies do not establish efficacy or comparative superiority. Based on data obtained from a large wound-care–specific Electronic Medical Record (EMR) database (WoundExpert®, Net Health, Pittsburgh, PA). Data are from January 1, 2014, through December 31, 2014.
Apligraf has been proven to reduce VLU and DFU burden on patients as well as healthcare costs
Explore the economic burden of VLUs and DFUs, or contact an Organogenesis Tissue Regeneration Specialist to see how Apligraf can be cost-effective.
Contact usPlease refer to the Apligraf Package Insert for complete prescribing information.
REFERENCES:
- Marston WA, et al. Wound Repair Regen. 2014;22(3):334-340.
- Treadwell T, et al. Adv Wound Care. 2018;7(3):69-76.
- Sabolinski ML, et al. J Comp Eff Res. 2018;7(8):797-805.
- Kirsner RS, et al. Wound Repair Regen. 2015;23(5):737-744.